

In a recent fivethirtyeight podcast, political scientist Dan Chen noted that in China the population largely distrusts local authorities’ response to the COVID19 pandemic, while placing faith in the large central government. Host Galen Druke then noted that in the United States, at least over the past few months, the reverse is true: support for local governments’ COVID responses is quite high while many judge the federal government’s response dimly.
One hundred years ago, the federal government largely abdicated its responsibility and placed much of the burden of fighting the influenza pandemic—which took 675,000 lives between January 1918 and April of 1919—on states and municipalities. Some of today’s governors and mayors have thus far demonstrated competence and leadership, and others have not. The same was true in 1918, and the list of the dead demonstrates that a nation on wartime footing battles pandemics very poorly, particularly at the federal level. The total war of “the war to end all wars” differed greatly from the conflicts we fight today with an all volunteer army; during the former all policies and institutions focused on its prosecution at the expense of everything else and measures established to facilitate mobilization and troop shipment overseas greatly exacerbated influenza’s spread. If not for the efforts of the American Red Cross along with Progressive-era volunteer social welfare organizations, the death toll would have been even worse.
The War and The Federal Government
Urban America was largely left to fend for itself in 1918. The federal government focused intensely on fighting in World War I and willfully ignored the pandemic. With a handful of exceptions, like Army Surgeon General William C. Gorgas, who sounded numerous alarms regarding the pandemic’s spread, officials purposely downplayed and ignored the illness.[1]
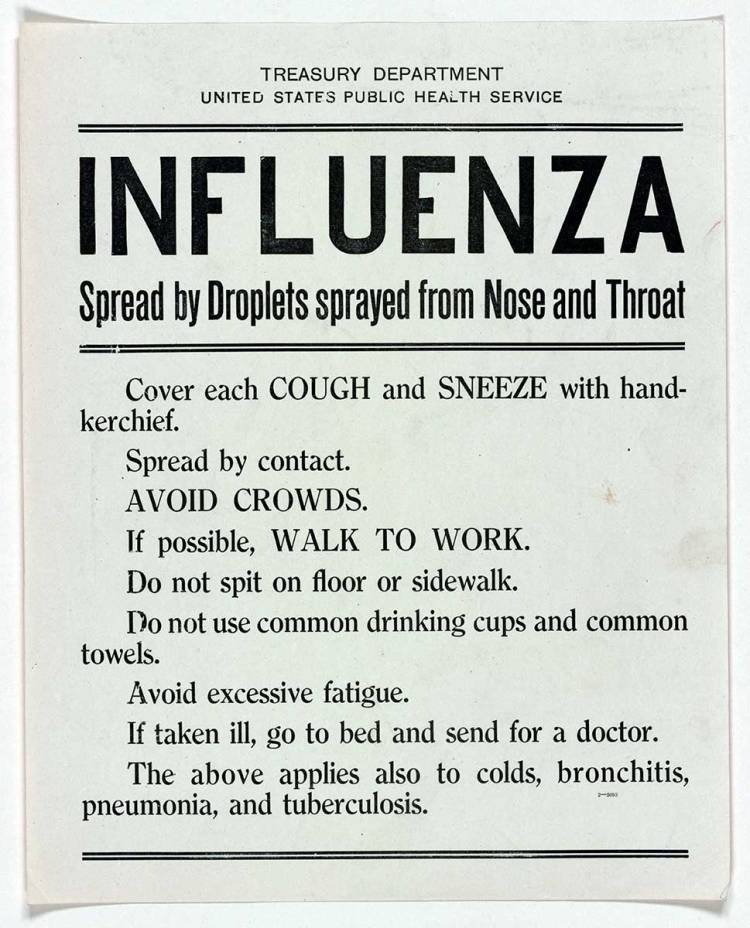
Cowed by the Espionage Act of 1917, the Sedition Act of 1918, and the overheated nationalism of the war, newspapers self-censored and avoided reporting on the illness, lest it reflect poorly on the mobilization of U.S. armed forces. Though as historian Alex J. Navarro pointed out in a recent interview, to say newspapers ignored the pandemic would be misleading: “Newspapers featured daily articles on the epidemic, often with front-page and above-the-fold coverage.” When they did address health, newspapers frequently offered little more than popular bromides: “Remember the three C’s, clean mouth, clean skin, and clean clothes … Keep the bowels open. Food will win the war … Help by choosing and chewing your food well.”[2] According to Navarro this was not intentional, but rather “a result of the knowledge gap that existed about influenza at the time.” Public officials frequently downplayed the virus unaware of its novel origins.

The pandemic came in three successive waves during a roughly nine-month period, with start- and end-points depending on geographical location. The initial wave of the virus was significant, but not as lethal as the two that followed. “High morbidity but low mortality,” marked the initial outbreak that lasted from Spring – Summer 1918. The latter two stretched from Summer – Fall 1918 and Winter 1918-1919 respectively, with the second wave the worst of the three. [4]
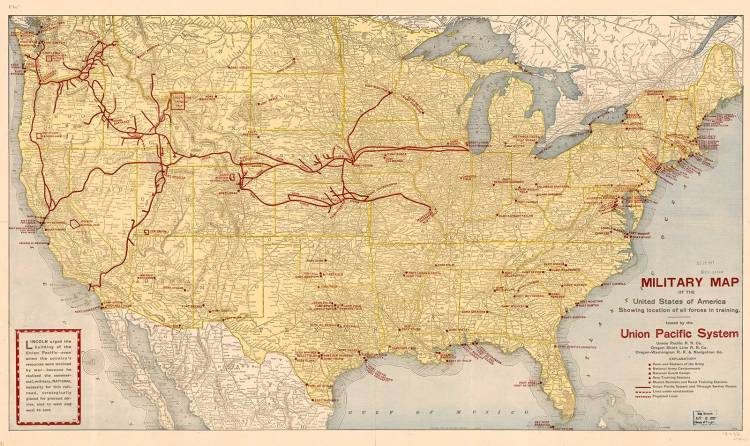
Fittingly, since the virus broke out in military camps before spreading into civilian communities and cities, army records offer important data points in studying the virus. The first wave of the disease emerged in Haskell County, Kansas, and soon after it exploded at Camp Funston (Fort Riley, KS). Much the same occurred in camps across the country: Camp Meade served as the entry point of the disease in Maryland, affecting both Baltimore and the capital; Camp Dix fed Philadelphia’s particularly brutal experience with influenza; Camp Devens helped inflame the outbreak in Boston; Camp Lee did the same outside Richmond; and the list goes on.[5]
Medical staff was in short supply. In most cities, between one quarter and one third of physicians and nurses had been swooped up by mobilization.[6] At the height of the pandemic in New York City, desperate and frightened citizens detained nurses by force.[7]

The American Red Cross (ARC) sent 9,000 nurses overseas. Domestically, it proved equally important. Its 3,864 local branches worked with local municipal governments and volunteer social welfare organizations in battling influenza. Well before the government, the ARC organized itself to fight what it feared would be an epidemic. They identified 6,000 Public Health Nurses to provide health care on the home front, comprised largely of “home defense nurses.”[8] Professionally trained but having been prevented from military service due to “physical disability, marriage or other causes,” home defense nurses, and public health nurses more broadly, often attended to those who could not reach a hospital.[9] After all, great numbers of those who contracted the illness and later died from it never made it to a medical facility.
For African Americans in U.S. cities, black nurses, who were denied the opportunity to serve in the war by both the American Red Cross and government, crucially intervened by providing medical care to segregated communities. Established by Ada Thoms in 1917, the Blue Circle Nurses filled the gap created by discrimination.[10]
Cities
Influenza struck the nation everywhere, but it did not strike the United States equally. Many city governments collapsed in the face of the virus’s second wave, leaving the ARC and local volunteer organizations to tend to the ill.[11]

Eastern and Southern cities endured the worst of it: Boston, Pittsburgh, and Philadelphia got hit early and hard.[12] New Orleans endured the third-worst death rate of the epidemic; Richmond’s death rate ranked above that of most Southern and Midwestern cities but lower than many others on the East Coast. “[N]o amount of forethought, in the absence of a sufficient number of doctors and nurses, could have prepared us for the tidal wave of disease and death that all but overwhelmed the city,” observed Richmond’s health commissioner. Washington, D.C.’s outbreak proved to be one of more severe episodes in the nation.
Though not hit with the same ferocity as the East Coast, West Coast cities still suffered. In California, San Francisco endured the harshest encounter with the disease. Los Angeles, due to swift actions by the city council and public health leaders, dodged the proverbial bullet.[13] Considering the importance of local welfare organizations and the overwhelming role that women played in them (and in the larger war effort on the home front), it’s possible that Southern California’s more robust network of clubwomen helped mitigate some of the pandemic’s effects.
While the Midwest managed to avoid the harshest aspects of the pandemic, it still struggled. At one point in October 1918, patients with influenza at Cook County Hospital in Chicago suffered a nearly 40 percent mortality rate. Overall, the Windy City performed well, not far behind its rival to the south, St. Louis, though it hardly avoided the pandemic’s consequences. The bodies may not have piled up as they did on the East and West Coasts, but “they did still pile up,” writes Barry.
St. Louis proved to be the model for fighting the virus.[14] Dr. Max C. Starkloff, the city’s health commissioner, took decisive action. Having tracked the illness from its emergence in Boston in September, Starkloff and local ARC chairwoman Virginia C. Hammar met in early October. Hammar “tried to impress him with the importance of the impending epidemic,” historian Marian Moser Jones notes in her four-city study of ARC’s response to the pandemic. Three days after their meeting, Starkloff closed down the city. The ARC also distributed 1. 2 million copies of educational pamphlets providing basic information on influenza in several languages, including Polish, Russian, Yiddish, Hungarian, Italian, Czech, and Spanish.[15]
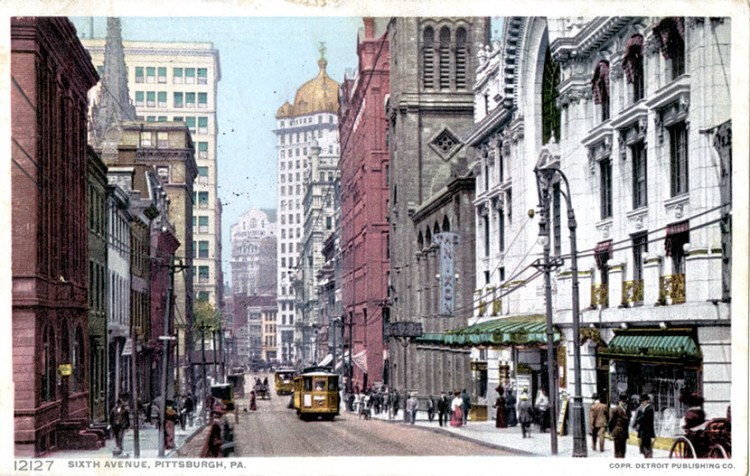
Though not in the Midwest, Pittsburgh also functioned well during the epidemic, planning in advance of the virus’s arrival in the city. Strategies were drafted and supplies and services were acquired by the local ARC chapter. As in St. Louis, it worked effectively with the municipal government.[16] However, it did not prevent great loss, as by some measures it recorded the highest death rate of any major American city, due in part to staggered social distancing measures and its notoriously poor air quality, which may have increased vulnerability among residents.
Metropolises governed by political machines varied in effectiveness. Dubbed the “worst governed city in America” by journalist Lincoln Steffens, Philadelphia’s Mayor Thomas B. Smith served as “chief lieutenant” to the Republican state machine run by state senator Edwin Vare.[17] Director of the Philadelphia Department of Public Health and Charities, Dr. Wilmer Krusen, a political appointee, lacked knowledge or expertise in public health and demonstrated no sense of urgency or alacrity. “Krusen offered civilian residents the soothing statement that they had nothing to fear so long as influenza cases were strictly isolated,” notes the Influenza Encyclopedia, an online database exploring the 1918-1919 epidemic. But “Krusen was terribly wrong.” His indecision, coupled with the reality that political power in the city was diffuse—Philadelphia’s municipal leadership divided its authority between Vare, precinct captains, and the mayor’s office—helped to lay the groundwork for one of the worst cases of influenza in any major city. The municipal government “did not wish to act, nor could it if it chose to,” notes Barry.[18]

In New York, Tammany Hall had regained control of the city government and purged its widely respected Department of Public Health, removing recognized public health experts and replacing them with patronage hires. By 1918, it had established itself as one of the best municipal public health agencies in the world, machine politics, however had placed at the head of its leadership individuals with no belief in modern science and whose only ambition aligned with politics rather than public health.[19] While political interference probably made the situation worse, the city’s tradition of managing infectious disease through surveillance, isolation, and quarantine appears to have prevailed. New York managed one of the lowest death rates on the East Coast.
Nationalistic fervor for the war served as one of the virus’s “superspreaders” in several cities. During World War I, the government mounted four Liberty Loan Drives to promote the sale of war bonds, ultimately raising $20 billion. Many cities held or had scheduled Liberty Loan Parades for late September or early October. Afterwards, each city suffered severe outbreaks. During San Francisco’s parade, 150,000 people gathered in Golden Gate Park. While its role as a major port also contributed, the parade seeded the virus and San Francisco endured the worst outbreak of any city in California or the West Coast. Within three days of Philadelphia’s parade, every bed in all of its 31 hospitals was occupied. Desperate residents offered nurses $100 bribes to gain admittance.[20]
In contrast, Los Angeles cancelled it’s own parade and managed to greatly reduce its casualties from the pandemic.[21] A testament to the sort of whiplash confusion that the virus sowed in local governments, just two days before the city council passed an ordinance shuttering “any place of public resort” and cancelling the parade, the city’s public health director told residents, “If ordinary precautions are observed there is no cause for alarm.”[22] The smaller and more remote city of San Diego fared best of the three big California metropolises; its city board of health closed places of public gathering a few days after Los Angeles on October 13.[23]

With a few exceptions, such as the Los Angeles Theater Owners Association and the Church of Christ, Scientist, little resistance to the new restrictions surfaced in Southern California.[24] When it did, such as in less affected San Diego, municipal leadership responded unequivocally. “There is a class of people blind and indifferent to the death and sick rate, apparently unconcerned about everything but nickel nursing and sight-seeing,” San Diego Mayor George Marston remarked in his endorsement of the city’s quarantine. “If we cannot put life and health above dollars and pleasure for a few days, we had better abolish the Bible and the Constitution.”[25]
Besides quarantines, many public health officials endorsed the use of masks. Skepticism regarding their efficacy followed in some quarters. “Modern civilization has abolished the mask as a part of human wearing apparel … only highwaymen, burglars, and hold up men wear masks professionally,” argued the San Diego Union in an editorial. “We sincerely regret … that some of the younger women in public employment are compelled to wear these masks. We miss the pretty faces….” Only a few weeks later, when deaths began to mount, the newspaper changed course and blamed “Los Angeles immigration” to San Diego as a prime culprit in the pandemic’s local spread.[26]
City and state officials throughout Northern California deployed the rhetoric and patriotism of the war to convince residents of masks’ necessity, but such appeals failed to convince everyone. In San Francisco the Anti-Mask League formed to protest an October 24, 1918 ordinance requiring their use. The local ARC attempted to combat such attitudes. “A week ago I laughed at the idea of the mask … I wanted to be independent. I did not realize that the cost of such independence was the lives of others,” its chairman told journalists. In one incident, a man refusing to wear a mask shot three people in an altercation.
The effectiveness of masks remains in debate. In his 1989 work, Epidemic and Peace, 1918, Alfred Crosby Jr. argued that any decline that occurred in San Francisco’s influenza rate had less to do with masking and more to do with the influenza’s declining strength.[27] Other historians such as John Barry also note that masks, though still advisable, may not have been as effective a barrier against transmission and that influenza strength did decline after the second wave. However, Crosby also asserted that cities with stricter closing orders fared no better or worse than others who adopted fewer precautions; a point that appears far more debatable in the decades since the book’s publication, during which time a great number of studies have been produced refuting this argument—particularly considering advances made in our understanding of the impact of environmental factors on mortality.[28]
Race
Though the dearth of record keeping prevents any authoritative conclusions, evidence suggests African Americans may have suffered far fewer casualties from the pandemic. Undoubtedly, African Americans were denied the same access and level of health care available to whites, but during the progressive era a network of black hospitals arose in several cities: Tuskegee Institute Hospital and Nurse Training School in Tuskegee, Alabama (1892); Frederick Douglass Memorial Hospital and Training School in Philadelphia (1895); Home Infirmary in Clarksville, Tennessee (1906); and Provident Hospital in Baltimore (1894) serve as a few examples.[29]

Additionally, like their white counterparts, black clubwomen attempted to address health disparities within their communities.[30] For example, in Atlanta African American clubwomen established the Atlanta Neighborhood Union in 1908, a settlement house that operated a health center and served as a focal point for community health and sanitation initiatives. The Woman’s Improvement Club took the lead in anti-tuberculosis efforts in Indianapolis in 1905.[31]
Despite obvious inequalities, major African American newspapers such as the Chicago Defender and Philadelphia Tribune suggested the pandemic’s impact had been muted. On October 12, as Philadelphia groaned underneath the weight of the epidemic, the Tribune wrote that while “hundreds are lying now at the point of death, colored and white … There seems to be more influenza and deaths among white people than the colored people.” The Defender and Baltimore Afro-American printed similar accounts.[32]
Then again, one must remember that if the white press felt it necessary to self-censure and avoid influenza coverage so as not to distract from the larger war effort and align with nationalistic impulses, black newspapers dealt with similar pressures. To what extent, black media coverage reflects the same imperatives toward wartime reporting maintained by its white counterpart remains hard to say. Though the black press had debated the efficacy of fighting World War I in light of discrimination, it was no less invested in American victory. After all, for civil rights leaders such as W.E.B. DuBois and Charles Hamilton Houston, the war offered a chance to gain the rights of citizenship long denied Black Americans.
Death records support that African Americans perished at a lower death rate. For example, in Philadelphia, then the northern city with the largest black population, between September 20, 1918 and November 8 there were 11,875 white residents who died from the pandemic while only 812 African Americans succumbed to the disease.[33] Chicago’s white population witnessed a 2,610 percent increase in deaths from the previous year while its black community saw an increase of 1,400 percent. Chicago’s department of health concluded that African Americans were “more immune” than their white peers.[34]
What explains this discrepancy, especially when one considers environmental factors related to segregation and discrimination? First, it’s very possible that official reports under counted the number of black deaths due to the virus. Second, scholars like Crosby argue African Americans were more subject to infection during the first wave due to the aforementioned inequalities and thereby had built up immunity when the disease had been milder, protecting them against the later, more severe strains. Third, segregation might have perversely operated as a “de facto quarantine,” noted public health care expert Vanessa Northington Gamble in a 2010 study on the subject.[35]
For good and for ill, American federalism took center stage during the influenza pandemic of 1918-1919. Out of necessity, state and municipal governments took the reigns with varying levels of success and failure, though even in the best cases, the results were dire. A concerted federal effort might have prevented the death toll rising to 675,000, but that was not in the cards. To paraphrase Tip O’Neill, all politics is local, nevermore so than during a pandemic, apparently.
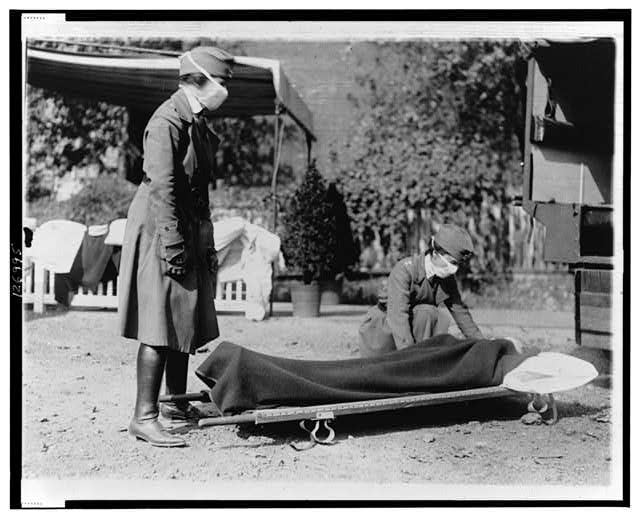
Featured image (at top): “The Red Cross Emergency Ambulance station of the District of Columbia Chapter is usually a busy place. But during the influenza epidemic of the autumn of 1918 it was worked over time,” 1918, Prints and Photographs Division, Library of Congress.
[1] John M. Barry, The Great Influenza: The Story of the Deadliest Pandemic in History, (New York: Penguin House, 2018), 384-88.
[2] Barry, The Great Influenza, 339.
[3] N. Pieter M. O’Leary, “The 1918-1919 Influenza Epidemic in Los Angeles,” Southern California Quarterly Vol. 86 No. 4 (Winter 2004): 394.
[4] David M. Morens and Anthony S. Fauci, “The 1918 Influenza Pandemic: Insights for the 21st Century,” The Journal of Infectious Diseases Vol. 195 No. 7 (April 1, 2007): 1023.
[5] Kathleen M Fargey, “The Deadliest Enemy,” Army History, No. 111 (Spring 2019), 28; Barry, The Great Influenza, 187; Richard H. Peterson, “The Spanish Influenza in San Diego, 1918-1919,” Southern California Quarterly Vol. 71 No. 1 (Spring 1989): 91.
[6] Barry, The Great Influenza, 318.
[7] Barry, The Great Influenza, 277.
[8] Marian Moser Jones, “The American Red Cross and Local Response to the 1918 Influenza Pandemic: A Four City Study,” Public Health Reports Vol. 125 No. 3 (April 2010): 92-104.
[9] Arlene W. Keating, “’Alert to the Necessities of the Emergency’: U.S. Nursing during the 1918 Influenza Pandemic,” Public Health Reports Vol. 125 No. 3 (April 2010): 107-108.
[10] Keating, “’Alert to the Necessities of the Emergency’,” 107-108.
[11] Barry, The Great Influenza, 373, 395-396.
[12] Barry, The Great Influenza, 373.
[13] O’Leary, “The 1918-1919 Influenza Epidemic in Los Angeles,” 394.
[14] Moser Jones, “The American Red Cross and Local Response to the 1918 Influenza Pandemic: A Four City Study,” 98-100.
[15] Moser Jones, “The American Red Cross and Local Response to the 1918 Influenza Pandemic: A Four City Study,” 98, 100.
[16] Jones, “The American Red Cross and Local Response to the 1918 Influenza Pandemic: A Four City Study,” 98, 100.
[17] Barry, The Great Influenza, 198-199.
[18] Barry, The Great Influenza, 200.
[19] Barry, The Great Influenza, 268-9.
[20] Barry, The Great Influenza, 220.
[21]O’Leary, “The 1918-1919 Influenza Epidemic in Los Angeles,” 394.
[22] O’Leary, “The 1918-1919 Influenza Epidemic in Los Angeles,” 394; Barry, The Great Influenza, 336.
[23] Peterson, “The Spanish Influenza in San Diego, 1918-1919,” 92.
[24] O’Leary, “The 1918-1919 Influenza Epidemic in Los Angeles,” 397-398
[25] Peterson, “The Spanish Influenza in San Diego, 1918-1919,” 96.
[26] Peterson, “The Spanish Influenza in San Diego, 1918-1919,” 95,99.
[27] Alfred Crosby, Jr., Epidemic and Peace, 1918 (Westport, Conn.: Greenwood Press, 1976), 105, 109.
[28] Crosby, Jr., Epidemic and Peace, 1918, 74, 101.
[29] Vanessa Northington Gamble, “’There Wasn’t a Lot of Comforts in Those Days’: African Americans, Public Health, and the 1918 Influenza Epidemic,” Public Health Reports Vol. 125, No. 3 (April 2010), 115-116, 119.
[30] Glenda Gilmore, Gender and Jim Crow: Women and the Politics of White Supremacy in North Carolina, 1896-1920, (Chapel Hill: University of North Carolina Press, 1996).
[31] Gamble, “’There Wasn’t a Lot of Comforts in Those Days’,” 116.
[32] Gamble, “’There Wasn’t a Lot of Comforts in Those Days’,” 119.
[33] Gamble, “’There Wasn’t a Lot of Comforts in Those Days’,” 120.
[34] Gamble, “’There Wasn’t a Lot of Comforts in Those Days’,” 120.
[35] Gamble, “’There Wasn’t a Lot of Comforts in Those Days’,” 120.
